Aspirin Modes of Action and Clinical Benefits: What We Know Today CME
Karsten Schrör, MD
Introduction
Aspirin (acetylsalicylic acid) is among the most widely used anti-inflammatory analgesics and its benefits at doses of ≥300 mg are well established. It is also effective at lower doses (≤100 mg/day) in the secondary prevention of cardiovascular disease (CVD).[1-12]
Its use is widely recommended in treatment guidelines. Furthermore, aspirin has shown significant benefit in patients with gastrointestinal (GI) cancers, most notably colorectal cancer (CRC),[13] and the United States Preventive Services Task Force (USPSTF) has recently made a draft recommendation for the use of aspirin in the prevention of CVD and cancer.[14]
Randomized studies suggest that low-dose aspirin is beneficial in the primary prevention of CVD, and evidence is growing for a role in the prevention of other cancers of the Gl tract and improving survival after a cancer diagnosis.[3-7,15-17] This article will review the modes of action of aspirin and describe its benefits in various conventional and new therapeutic indications.
Mechanism of Action
Aspirin acetylates and thereby modifies the activity of enzymes. This acetylation is irreversible; ie, it changes the enzymatic properties of the targeted enzyme throughout its lifetime, which is in most cases much longer than the half-life of unmetabolized aspirin in blood -- approximately 30 minutes.
This acetylating property of aspirin is unique among nonsteroidal anti-inflammatory drugs (NSAIDs).[3,18-21] Cyclooxygenases (COXs) are the major target of aspirin at low, antiplatelet doses (75 to 325 mg/day). The acetylation of COX-1 prevents the production of prostaglandins (PGs) and thromboxane A2 from arachidonic acid. The acetylation of COX-2 also reduces PG production, but mainly changes the activity of the enzyme from a COX to a lipoxygenase that produces "aspirin-triggered lipoxin" (ATL) through interaction with white cell lipoxygenases.[22] 15-epi-lipoxin A4 is a constitutive protective lipid that helps to maintain a healthy cardiovascular (CV) system, to reduce acute inflammatory responses, and to improve tissue healing.[21] Aspirin is more potent at inhibiting COX-1 than COX-2.
The ability of aspirin to acetylate (inhibit) COX-1 and subsequent thromboxane formation has been suggested as the primary mechanism of antiplatelet action.[23,24] However, the clinical effects of aspirin cannot be solely ascribed to the inhibition of COX-1 in platelets, and subsequent platelet secretion and aggregation.
They also involve paracrine actions of platelet secretion products, such as sphingosine-1-phosphate (S1-P), inflammatory mediators, or mitogens on other cells; for example, white cells and endothelial cells, as well as other acetylation targets relevant for inflammation, thrombosis, and tumorigenesis (Figure 1).[19,20,25-30]
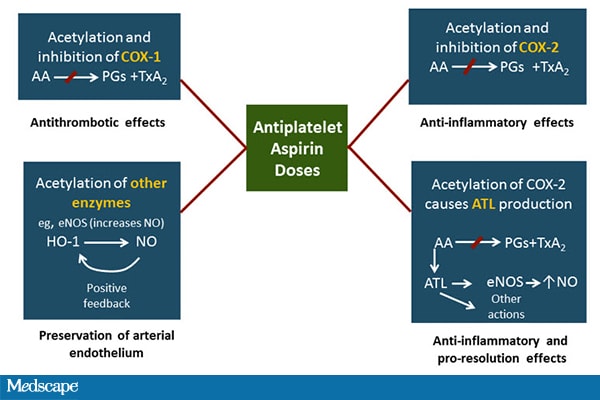
AA = arachidonic acid; ATL = aspirin-triggered lipoxin; COX = cyclooxygenase; eNOS = endothelial nitric oxide synthase; HO-1 = heme oxygenase-1; NO = nitric oxide; PG = prostaglandin; TxA2= thromboxane A2.
Role of Asprin in Cardiovascular Disease
Secondary Prevention of Cardiovascular Disease
The benefits of low-dose aspirin (≤100 mg once daily) in the secondary prevention of CVD are well established, and it has been shown to reduce the risk of major CV events -- nonfatal myocardial infarction (MI), nonfatal stroke, or death from vascular causes -- by approximately 22%.[6]
Low-dose aspirin is widely recommended in treatment guidelines as first-line therapy for the secondary prevention of CVD following MI, acute coronary syndrome (ACS), and interventions such as the insertion of stents.[1-12] There is an increased risk of GI and extracranial bleeding with aspirin.
The mechanisms for upper GI bleeding are not well understood, but are essentially related to the antiplatelet effects of aspirin and its interference with the coagulation process that is initiated by platelets.
Whether enhanced GI bleeding is also affected by the local irritating effects of aspirin on the stomach mucosa and the inhibition of local PG biosynthesis remains a matter of discussion.[32]
However, in secondary prevention, the number of patients who avoid a serious CV event is significantly greater than those who experience bleeding (risk/benefit ratio 10:1).[20,33] Recommended dosages are mostly in the range of 75 mg to 100 mg aspirin/day. Aspirin is also an integral part of dual antiplatelet therapy with prasugrel, ticagrelor, or clopidogrel.[3,12,34]
Research is ongoing into the optimal aspirin dosage and new approaches to antithrombotic prevention. In this context, new and exciting findings have been reported for aspirin in the prevention of primary and secondary venous thromboembolism (VTE; EPCAT and INSPIRE studies).[35, 36]
The EINSTEIN-CHOICE study will provide new insights into the optimal antithrombotic strategy for extended VTE treatment by comparing 2 doses of rivaroxaban with aspirin.[37]
Primary Prevention of Cardiovascular Disease
The benefits of low-dose aspirin in the primary prevention of CV events are less clear than for secondary prevention because the risk of a CV event is lower than in secondary prevention, whereas the risk of bleeding is similar.[3-7,15,16]
Therefore,in order to optimize the risk/benefit ratio, physicians need to assess the patient's baseline risk of future CV events and balance it against the risk of future bleeding.
The most important risk factors include preexisting diseases, in particular hypertension, hypercholesterolemia, and diabetes, a history of peptic ulcers, older age, and concomitant use of NSAIDs.
Preventive strategies to reduce the risk of bleeding in the upper GI tract include the use of gastroprotective agents, such as proton pump inhibitors, and debatably, the eradication of Helicobacter pylori.
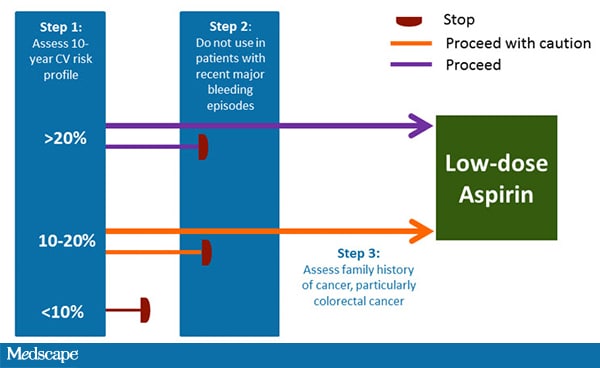
Several guidelines recommend the use of low-dose aspirin in patients with an increased risk for CV events[4,17,38]; for example, the European Society of Cardiology recommends that those with a 10-year CVD risk of >20% take daily aspirin (Figure 2).
If the risk is <10%, other factors should be taken into account. The beneficial effects of aspirin are similar in patients with or without diabetes, and between sexes, and 'aspirin-resistance' due to an insufficient pharmacological activity of aspirin is thought to occur rarely.[17,20] However, clinical treatment failures may occur for several reasons, including delayed absorption with enteric-coated tablets allowing for enhanced metabolic degradation of aspirin especially at low doses,[39] drug interactions with NSAIDs, and platelet stimulation by non-aspirin-sensitive stimuli are thought to account for most instances of 'aspirin resistance'.[40] In addition, in situations with increased platelet turnover rates, such as diabetes, twice-daily dosing has been shown to be more effective than once-daily dosing, probably because of more rapid replacement of aspirinized platelet COX-1 by fresh platelets from the bone marrow.[41,42]
Three ongoing larger-scale trials are evaluating the effects of aspirin use in higher-risk populations: ASPirin in Reducing Events in the Elderly (ASPREE),[43] A Study of Cardiovascular Events iN Diabetes (ASCEND),[44] and Aspirin to Reduce the Risk of Vascular Events (ARRIVE).[45]
Primary Prevention of Cancer
There is increasing evidence of the benefits of low-dose aspirin in the prevention of cancers, in particular CRC, but also other solid tumors of the GI tract (Table).
The majority of the data come from secondary analyses of trials that studied the role of aspirin in reducing the risk of CV events.[13,15]
In September 2015, the USPSTF has made a draft recommendation for the use of aspirin in the primary prevention of CVD and CRC in people aged 50 to 59 years whose 10-year CVD risk is 10% or greater, who are not at increased risk for bleeding, who have a life expectancy of at least 10 years, and who are willing to take daily low-dose aspirin for at least 10 years.[14]
However, most guidelines do not reflect the growing evidence base, so physicians should take the individual patient risk/benefit ratio into account when deciding whether or not to prescribe aspirin in primary prevention.[3]
Colorectal Cancer
Evidence for the chemopreventive effects of aspirin is strongest for CRC; for example, a randomized controlled trial (RCT) of patients with Lynch syndrome, an inherited condition that increases the risk for developing CRC, found that 600 mg aspirin once daily reduced the incidence of CRC.
A first tendency for this became apparent 3 to 4 years after the start of aspirin therapy and became significant in an "on treatment" analysis after 56 months.[46]
Numerous observational trials suggest that regular, long-term intake of low-dose aspirin (≤100 mg/day) significantly reduces the risk of CRC and may also prevent the appearance of distal metastases and prolong survival in certain patient subpopulations.[47]
Aspirin has demonstrated a delayed action (at least 3 to 5 years) for reducing the risk of colon cancer.[15,48] Aspirin treatment for up to 20 years reduced the risk of proximal colon cancer by 55%, but did not change the incidence of distal colon cancer.[48]
Importantly, low-dose aspirin (75 mg daily) was just as effective as higher doses in reducing the risk of cancer.[48] The reason why aspirin may affect proximal colon cancer preferentially may be due to its less complete inhibition of COX-2 in distal tumors.[48]
Another interesting finding was a reduced total mortality that was due to reduced non-CV mortality; ie, probably due to reduced cancer mortality.[13]
COX-1 inhibition prevents thromboxane formation as well as the secretion of several platelet-derived products that might act as paracrine mediators on other cells.[20]
Sphingosine-1-phosphate (S1-P) is a lipid mediator with proinflammatory and oncogenic activities that also induces COX-2 in nucleated cells.[49]
In blood, S1-P is stored in platelets and released during platelet stimulation in a thromboxane-dependent manner, and may be involved in tumor growth.
Low-dose aspirin treatment prevents S1-P release from human platelets.[50] It is unlikely that all of the chemopreventive effects of aspirin in CRC are solely due to platelet-related actions. One mechanism proposed for aspirin's antitumor activity involves the mammalian target of rapamycin (mTOR) pathway, which is progressively dysregulated in colorectal tumorigenesis, suggesting that aspirin's antitumor activity is due to its potent inhibition of mTOR signaling and its activation of AMP-activated kinase, which also inhibits mTOR and protein synthesis.[51]
However, it should be noted that these and many other antitumor effects of aspirin, such as interaction with certain transcription factors (eg, NFkB or S56-kinase), are mainly seen in cell culture studies at high aspirin/salicylate levels that might completely block cellular oxidative phosphorylation (ie, energy metabolism and all ATP-dependent cellular signaling).[52] If the full chemopreventive action of aspirin is seen at 75 mg/day, these actions are probably not involved.
COX-2 is an inducible enzyme that is upregulated in CRC. Of the various PGs produced by COX-2, PGE2 is involved in tumorigenesis, inhibits apoptosis, and has proinflammatory and immunosuppressive effects.[18] PGE2 stimulates tumor angiogenesis and proliferation, as well as distant metastasis, possibly via vascular endothelial growth factor (VEGF). VEGF is the most relevant angiogenic factor with more than 80% of VEGF in blood being stored in platelets.[53]
Aspirin also upregulates NSAID-activated gene-1 (NAG-1), which may act as an inhibitor of tumor formation.[18] Some cancer cell lines do not have COX-2, but aspirin is able to inhibit proliferation and induce apoptosis associated with an inhibition of β-catenin-dependent gene transcription, although only at extremely high concentrations.[18] Thus, the antiapoptotic/antitumor actions of aspirin may be a combination of effects, with acetylation of COX-1, COX-2, and perhaps, additional factors inhibiting carcinogenesis and tumor metastases.[20, 21]
Other Cancers
Aspirin reduced cancer deaths by approximately 15% when 51 RCTs assessed the time course of the risk/benefit profile of daily, low-dose aspirin on cancer incidence, mortality, and non-vascular death.[13] This was particularly noticeable from 5 years onwards (37% reduction).
The effect of aspirin on cancer incidence increased with the length of therapy. In contrast, the effect of aspirin on major vascular events and major extracranial bleeding diminished over time.[13] Aspirin also reduced cancer metastasis, which could account for the early reduction in cancer deaths observed in some clinical trials.[54]
Observational studies suggest that aspirin reduces the risk for several other cancers (esophageal, gastric, biliary, prostate, lung, and breast cancer) and the risk for distant metastasis (Table).[14,55,56] However, the effects on non-GI cancers were very small and not seen in all trials (eg, breast cancer).[57] Thus, until interventional studies are conducted with low-dose aspirin, the data remain inconclusive.[56]
Condition Incidence Estimated Risk Ratio Mortality Estimated Risk Ratio
Myocardial infarction 0.82 0.95
Stroke 0.95 1.21
Colorectal cancer 0.65 0.60
Esophageal cancer 0.70 0.50
Gastric cancer 0.70 0.65
Lung cancer 0.95 0.85
Prostate cancer 0.90 0.85
Breast cancer 0.90 0.95
Best estimates of incidence and mortality are shown. Refer to original article for conservative estimates.[15]
Aspirin for the Treatment of Cancer
There is growing epidemiological evidence to support the beneficial effects of taking aspirin after a cancer diagnosis in order to prevent metastases and prolong survival, in particular for CRC and GI cancers.[58-61]
A number of trials are ongoing or planned that aim to establish a role for aspirin in the treatment of cancer.[62,63] Research is also ongoing into specific tumor mutations as potential biomarkers of aspirin response.[64]
Prevention of Other Diseases/Conditions
Patients With Cognitive Decline
Observational studies have suggested that the use of long-term NSAIDs may delay the progression of dementia. By reducing the number of sub-clinical brain infarcts/ischemia, aspirin could have a beneficial role in delaying cognitive decline.[65-68] Also, platelets are a major storage site for amyloid-ß and are hyperactive in Alzheimer’s disease.[69,70] However,the data are currently inconclusive.
Additional well-designed studies will help elucidate the role of aspirin in cognitive function.
Patients With HIV-1 Infection
Patients with human immunodeficiency-1 virus (HIV-1) infection have an elevated CV risk, and platelet activation causing a prothrombotic state may be a significant factor in these patients. Aspirin is likely to have a beneficial role by inhibiting platelet activation.
Between 6% and 15% of HIV deaths are due to CVD, including coronary heart disease and MI.[71-74] In addition to pathological immune reactions, patients with HIV infection also have platelet hyperreactivity and endothelial dysfunction, which can be attenuated after low-dose aspirin.[71,75].
There is also a growing body of evidence that HIV infection is associated with heightened immune activation and a chronic inflammatory state.[76-78]
Short-term studies suggest that low-dose aspirin may therefore have a role in attenuating platelet activity and immune activation, and longer-term studies on this are ongoing.[79,80]
Patients With SIRS
Patients with systemic inflammatory response syndrome (SIRS) may also benefit from early aspirin treatment. As with other indications, platelets are likely to have a key role in these pathologies, and there is evidence of the beneficial effects of aspirin and other antiplatelet agents in these critically ill patients.[81-83]
Pre-eclampsia
Aspirin has been shown to reduce the risk of developing pre-eclampsia in women at high risk for the condition, and early low-dose aspirin is recommended by both the United States Preventive Services Task Force and the World Health Organization for such women.[38,84,85] Recently, it has been suggested that women at modestly elevated risk (6% to 10%) should also be considered for aspirin treatment. RCTs are needed to establish clear evidence of a benefit.[86]
Summary
Aspirin has shown benefits in the treatment of a wide range of conditions.
The evidence today is most robust for the secondary prevention of CVD, and although the use of aspirin for primary prevention is an area of intense debate, several treatment guidelines recommend its use in higher risk patients with a low risk for bleeding.
Clinical trial data also support the use of aspirin for the prevention of colorectal and other GI cancers, and data are emerging for a role for aspirin in the prevention of metastases after a cancer diagnosis in certain subpopulations of patients.
Although the USPSTF has made a draft recommendation for the use of aspirin in the primary prevention of CVD and CRC, the chemopreventive benefits of aspirin are not yet addressed in most treatment guidelines. A range of possible mechanisms for aspirin's anticancer action have been proposed.
An involvement of the antiplatelet effect is not unlikely as current evidence suggests a full chemopreventive effect already at antiplatelet doses. Aspirin also has a role in the management of other conditions, including immunomodulation in HIV, prevention of pre-eclampsia, treatment of SIRS, and possibly, prevention of cognitive decline.
The results of ongoing studies on the effects of aspirin across various conditions may help physicians to more accurately assess the risk/benefit ratios of aspirin use in individual patients and may also lead to the inclusion of aspirin in treatment guidelines for CRC.
